












Exclusive Article at EMRIndustry ..
By Donald M. Voltz, MD, Aultman Hospital, Department of Anesthesiology, Medical Director of the Main Operating Room, Assistant Professor of Anesthesiology, Case Western Reserve University and Northeast Ohio Medical University.
Board-certified in anesthesiology and clinical informatics, Dr. Voltz is a researcher, medical educator, and entrepreneur. With more than 15 years of experience in healthcare, Dr. Voltz has been involved with many facets of medicine. He has performed basic science and clinical research and has experience in the translation of ideas into viable medical systems and devices.
Thanh Tran, CEO of Zoeticx, Inc. also contributed.
This year’s medical student graduating class will be the first group of physicians trained without paper-based medical records. Healthcare workers understand the stated benefits of electronic health information, but most can share the scenarios I describe here.
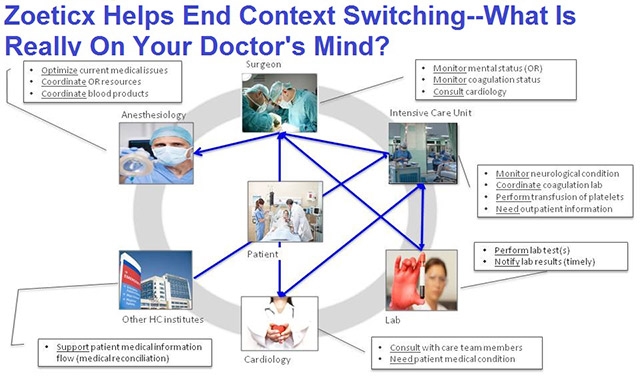
Mr. Jones is admitted to the intensive care unit with a possible cardiac condition. You spend close to one hour reviewing his medical history in the ER. Concerned with his EKG tracing and abnormal electrolytes, you admit him to the cardiac intensive care unit.
Later on the cardiac ICU pages you. The charge nurse in the ICU doesn’t know why you were paged and tracks down Mr. Jones’ nurse. She received a call from the lab about an elevation in his troponin level and wanted to advise you of his slowly declining blood pressure and increase in heart rate. She also mentioned that his EKG and chest x-ray have been completed and are in the ‘system’. You review the findings and create an assessment and plan.
Your computer requires you to connect to the VPN client and log into the hospital system. Once a secured connection has been obtained, a gateway into the EMR enables you to access his labs. Nothing ominous is identified so you navigate to the nurses’ flow sheet.
Navigating EMR Gulags
You begin dealing with the technical difficulties of the EMR application and the disparate pieces of data that summarize Mr. Jones physiologic state. Closing that EMR, you next connect to the radiology management EMR system to view his chest x-ray. A similarly slow process allows you access to his EKG, stored in yet another cardiology management EMR. After navigating three disparate EMRs, you make a diagnosis. A course of antibiotics is prescribed. You enter the orders into another EMR. Data is stored, transferred and acted upon in disconnected and unrelated systems.
Another healthcare provider receives a piece of information such as a set of vital signs or the result of a lab. If the information raises a question or necessitates a decision from a physician, a contact is made. The contact is often a manual one, using the antiquated paging system or some technological surrogate such as text messaging or a phone call. Given the demands of healthcare, irrespective of the method used to contact a physician, they are not always in a position to take the call or page when placed. They also may no longer be the responsible physician covering the patient, or they can’t respond immediately.
The Dizzying Pace of Context Switching
Although the specifics of this scenario vary with disease and patient, the flow of work, even in today’s EMR-centric health systems, is similar for most medical pros. The issue many of us are aware of, and recognize in the flow of information, is context switching. In the cases described, the nurse’s and physician’s workflow has been interrupted, and they need to switch contexts from current tasks to respond to the current issue.
When the physician receives the call, message or page, the first context switch is required. The physician received a notification on a pager, but has no clue regarding the urgency of the page, unless an alpha numeric message came through. Often, the question being asked will require a collection of additional EMR based information in order to make the appropriate decision. This leads to another context switch, either requesting additional information from the nurse or logging into the EMR to gather recent trends or lab data.
Today’s EMR workflow doesn’t require a single context change, but multiple changes between unconnected EMR systems and personal, mobile communications devices. This disrupts all providers involved, along with requiring us to hold multiple, disconnected pieces of patient information in our minds while proceeding to gather information from different sources. Efficiency is impacted; work duplicated, and a higher probability for errors created or missing information that might have lead to a better outcome.
Paradigm Shift Required
To address these issues, we need a paradigm shift, a conversion of the stream of information for patient care. Despite some improvements in EMR technology, healthcare providers still need to search for information in these systems similar to a Google search. Pulling information out of various healthcare data management systems or from different portions of a single EMR takes time away from patients.
The problem is not a lack of technology to allow for data conversion. Medical pros need the simple type of push technology that is used to flag an article on newspaper web site, and receive notifications when a related article of interest is published. In addition, the ability to access related information in a single application or seamlessly move between applications is needed. This will reduce the switching of context and exists with smart phones and other mobile computing platforms.
To make this a reality for healthcare providers, hospitals need to consider new healthcare 2.0 solutions that address these needs. To build a more effective and efficient workflow in healthcare requires the integration of messaging, accessing data from disparate and disconnected health databases, all wrapped in a single view, secure platform, accessible by various smart computing devices.
Solutions Available
What is frustrating to physicians is that the pieces for creating such a system are currently available. One security software leader has developed a mobile security platform that enables secure transmission of data between mobile applications and web-based storage repositories, including servers, web-pages or other data portals.
Tapping into this platform, or other security wrappers will be significant given the sensitivity of the information being transferred. Although secured SMS messaging is available, exploring solutions that integrate with EMR’s and provide push notification is required to reduce or prevent the context switching issues that lead to distraction, inefficiencies and potential errors.
This scenario might appear to be aimed at physicians to selfishly improve their comfort level, but it is more about patient safety, quality of care and finally bridging the gap between EMRs and better patient outcomes. There needs to be a shift to a patient centric approach that connects all the points.
We need collaborative EMR systems that work like medical pros and include “smart” analysis that can interpret data. The information needs to be delivered to those who need it, when they need it, with all in one place. Add voice to text capability to save valuable physician and nurse time and help end miscommunications. Right now the only healthcare 2.0 solution that addresses all of these needs is a middleware based EHR connectivity system from Zoeticx. It offers an end to context switching and addresses security requirements.
The implications of a Zoeticx integrated EHR system that reduces context switching, promotes smart alerting and the pushing of relevant patient information to medical pros will impact patient satisfaction, address quality and timeliness for patients, and allow for more proactive care and patient follow up.



